
R.ALFRED for Autonomous Femur Fracture Reduction A procedure that demands both strength and precision
Femur fracture reduction is one of the most physically demanding tasks in orthopaedics. Surgeons must apply substantial traction to overcome strong counteracting muscle forces and realign long-bone fragments before fixation with plates or intramedullary nails. Even in experienced hands, perfect re-alignment on the first attempt is not guaranteed, often requiring repeated adjustments. Meanwhile, both patients and surgical teams can spend prolonged time under fluoroscopy, increasing cumulative exposure to X-ray radiation.

These challenges high forces, tight accuracy requirements, and radiation-heavy workflows make femur reduction a strong candidate for robotics. But there is a catch: the robot must be accurate and compliant at the same time. High precision is essential for alignment; high compliance is critical for safe interaction with the bone–muscle system.
The idea behind R.ALFRED
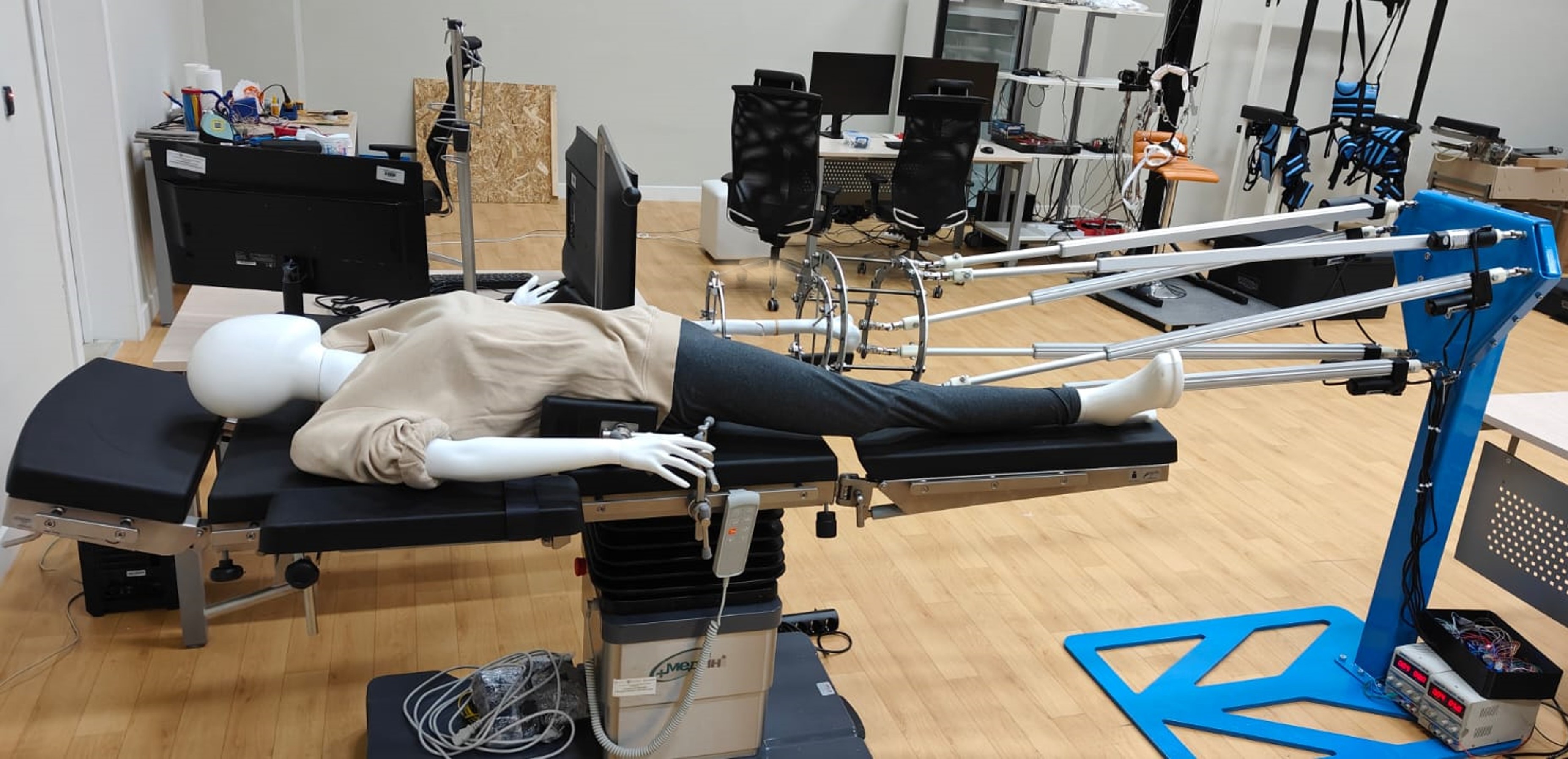
R.ALFRED (Autonomous Reduction of Femur Fractures) is proposed as a robotic system that supports orthopaedic teams during labor-intensive femur reduction while helping reduce time spent in radiation-stimulated environments. The approach centers on a 6-degree-of-freedom parallel robot, built not for brute force alone, but for controlled, safe, and adaptive reduction.
Instead of conventional stiff servo/DC motor actuation often associated with high endpoint impedance, R.ALFRED uses six intrinsically compliant actuators. This design choice is deliberate: compliance is built into the mechanics, reducing the risk of harmful interaction forces while still allowing the robot to generate the traction needed for long-bone alignment.
Designing for competing objectives
Femur reduction robotics lives in a world of competing requirements. A system must:
move with high kinematic accuracy,
transmit forces effectively with reasonable actuator loads, and
maintain interaction compliance for safety.
To navigate these trade-offs, the research formulated three design performance metrics:
Conditioning Index a measure linked to motion accuracy and stable force/torque transmission (an improved variant aligned with global conditioning concepts used in parallel robotics).
Actuator Force Index capturing how hard the actuators must work across operating conditions.
Interaction Compliance Index reflecting the robot’s ability to interact safely with the musculoskeletal environment.
Using these metrics, the team applied a multi-objective evolutionary optimization algorithm (SPEA2) to search the robot’s geometric design space. By varying key design variables, the optimization produced an optimal design that represents the best practical balance between accuracy, actuator demands, and compliance.
Proof of concept: control and trajectory accuracy
With the optimized design in hand, the project moved to initial validation. The robot was tested for trajectory-following accuracy, focusing on controlled rotational motions about three axes. A fuzzy-based closed-loop feedback controller was implemented to manage tracking performance under sinusoidal inputs.
The outcome: excellent trajectory tracking, demonstrating that the platform can follow commanded motions reliably an essential prerequisite before advancing to higher-level autonomy and force/compliance-controlled reduction strategies.
Where R.ALFRED goes next
R.ALFRED is designed with clinical realities in mind: reduction depends on anatomy, fracture type, and changing interaction forces. The next phase aims to upgrade the system from controlled motion to sensing-informed, surgeon-supervised autonomy:
Visual servoing and imaging integration: leveraging 2D X-ray images to reconstruct a usable 3D representation of the fracture for guidance and verification.
Biomechanical modeling: generating an optimal reduction path that minimizes error and respects physiological constraints.
Force/compliance-aware control: moving beyond pure position control to strategies that adapt to bone–muscle interaction feedback.
Optical stereoscopic tracking: mounting a stereo vision system to track the moving platform position/orientation in real time and automatically generate trajectories based on the current state.
Remote supervision: enabling the surgeon to supervise reduction with reduced exposure to radiation.

R.ALFRED represents a clear direction in next-generation orthopaedic robotics: not just automation, but safe autonomy, where compliance, accuracy, and adaptive control work together. If successful, the system could help replace traction-table based manual workflows with a platform that is repeatable, measurable, and less physically and radiologically burdensome for surgical teams.
Acknowledgment (clinical insight): The work recognizes clinical input on fracture reduction procedures received from Dr. Brendan Klar (Canberra National Capital Private Hospital, Australia).
